Understanding Heel Pain (Plantar Fasciitis)
June 1, 2026
Categories: Foot and Ankle, Rehabilitation Services
Tags: Plantar Fasciitis
What the Latest Clinical Guidelines Tell Us
Heel pain, often called plantar fasciitis, is one of the most common causes of foot pain seen in physical therapy. The 2023 updated Clinical Practice Guideline from the Journal of Orthopaedic & Sports Physical Therapy (JOSPT) helps clinicians use the most up-to-date evidence to diagnose and treat this condition more effectively.
What is Plantar Fasciitis?
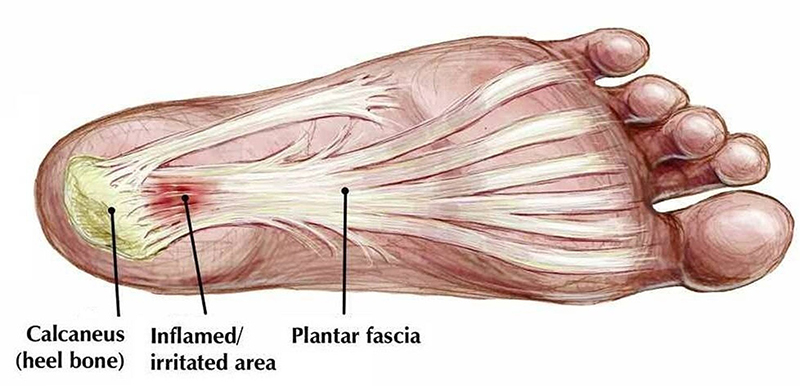
Plantar fasciitis is not considered solely an “-itis” in the classic sense of inflammation. Instead, it is better understood as irritation and overload of the plantar fascia, a thick band of tissue that supports the arch of the foot. Repeated stress, especially with standing, walking, running, or sudden activity changes, can lead to pain near the heel and within the arch of your foot.
How Clinicians Diagnose Plantar Fasciitis
The guideline emphasizes that diagnosis is primarily clinical, meaning it is based on:
- Pain at the bottom of the heel, especially with the first steps in the morning or after a period of rest
- Tenderness near the inside/front of the heel
- Symptom patterns that worsen with prolonged standing or activity
- Imaging (like MRI or X-ray) is usually not needed at first, unless symptoms are atypical or not improving.
Common Risk Factors for Planar Fasciitis
This guideline highlights several contributing factors that increase one’s risk for developing plantar fasciitis, including:
- Limited ankle flexibility (tight calf/Achilles complex)
- Higher body weight or recent weight changes
- Prolonged standing or walking occupations
- Running or sudden increases in activity
- Poor foot/ankle strength or mechanics
Importantly, many cases are multifactorial, meaning there is rarely just one cause!
What Treatment Works the Best (Based on Evidence)
The strongest recommendation in the guideline is that exercise-based physical therapy is the foundation of care:
Exercise Therapy (Most Important)
- Calf stretching
- Plantar fascia-specific stretching
- Progressive strengthening of the foot and calf
These help improve load tolerance and reduce recurrence.
Taping, Orthotics, Footwear Changes
- Short-term taping can reduce pain during flare-ups
- Prefabricated or custom orthotics may help some patients
- Supportive footwear can reduce strain during daily activity
These are typically adjuncts—not stand-alone cures.
Manual Therapy
Hands-on treatment may be used to improve mobility in the ankle and foot, especially when stiffness is present.
Education and Activity Modification
- The guideline notes limited or inconsistent benefits for:
- Avoid complete rest (which can worsen stiffness)
- Modify rather than stop activity
- Gradually increase load instead of sudden spikes
What is Not Strongly Recommended Alone?
The strongest recommendation in the guideline is that exercise-based physical therapy is the foundation of care:
- Steroid injections as a long-term solution
- Passive treatments without exercise (massage alone, ultrasound alone, etc.)
- Prolonged immobilization in most cases
The Key Message
Most heel pain improves with time, but recovery depends heavily on how the foot is progressively reloaded—not rested completely. It is important to note that this specific diagnosis can take some time to fully resolve in most cases.
The goal of rehab/treatment is not just pain relief, but restoring the foot’s ability to tolerate daily life, walking, and sport without recurring symptoms. A structured rehab plan combining stretching, strengthening, and a gradual return to activity is the most effective long-term approach for recovery. Contact Witham Rehabilitation Services or Witham Foot and Ankle to assist in your recovery!